Whirlwind of a week- #4
July 24th, 2018 by edwardchristiansen
What a whirlwind of a week, filled with numerous life-changing memories. The start of my week began on the Female ward and high care. I rounded with colleagues and made some med changes. One patient in particular, who is widely well-known in these parts, had end-stage kidney disease amidst other comorbidities. She is one of the fortunate few in the area who gets hemodialysis. Hemodialysis is what many people in the U.S. are familiar with for patients with renal failure. Blood is removed from the bloodstream, circulated through a dialysis machine to rid said blood of harmful waste-products, and returned/circulated back into the patient. Naturally, this process is incredibly expensive in resource allocation, educational requirement, among many other reasons. Recent budgetary reports put dialysis costs at approximately 1% of the medicare budget! It is estimated hemodialysis costs approximately $100,000 per patient per year. Around these parts, peritoneal dialysis is the mainstay. This patient was 68yo and had other comorbidities including hypertension, diabetes, and heart failure and had been recently discharged from a larger hospital. She had no way of making her many dialysis appointments due to social situations, and told her taxi driver to take her directly to Mseleni where she would naturally be admitted.

The problem patient
None of this would be an issue, however her physicians/medical team in the large city sent her with a list of items to be performed by her “primary care team.” Keep in mind where this hospital is, the types of cases were are facing, and the amount of assets available to us. The list was as follows:
- A CT scan of the chest in order to “rule out chronic lung disease”
- A non-emergent CT takes approximately 2-4 weeks to schedule and obtain here. An emergent takes 2-5 days!
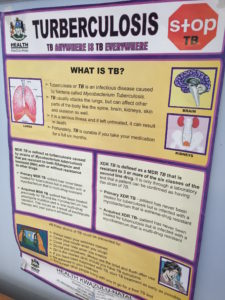
- I would also like to mention she had previously treated tuberculosis and, by definition, has chronic lung disease
- This test would NOT add to this patient’s quality of life, staging of disease, or life expectancy.
- A referral for pulmonary function tests
- Again, there is no benefit obtained from this set of tests
- A referral for a non-obstructed umbilical hernia to a general surgeon that has been present for 1 year
- This is something she could live with as it is not causing any pain, other problems, and is quite common.
We did order a repeat CXR which was compared to previous, looked at recent sputum samples that were obtained and negative for TB, as well as a blood test which confirmed a negative test for TB. Suffice it to say, we wrote a letter explaining the workup was a waste of resources and that it could be done at a later time at the patient’s discretion.

Comparing xrays
Tuberculosis is a global phenomenon and epidemic much decreased in the U.S. More than 2 billion people are estimated to be infected with M. tuberculosis. Per the WHO, in 2016 10.4 million individuals became ill with TB and 1.7 million died. Approximately 95% of TB cases occur in developing countries. It is largely associated with pulmonary(lung) component, however TB can occur anywhere. Nowhere is this more apparent here in South Africa. It was only in medical school textbooks and UWorld ?’s I saw central nervous system TB, skeletal TB, TB pericarditis(infection with TB affecting the fibrous sac around the heart, gastrointestinal TB, urogenital TB, etc. Here, numerous children develop the disease in some different manifestations but none more devastating to than skeletal deforming type. Children are frequently left immobile and the lucky ones get a wheelchair.
The rest of the week was a hodge-podge of everything. Thursday, I had the opportunity to spend the day in the OR or “theatre” as it is referred to here. After making ward rounds, Dr. Fredlund and I went to theatre. We had 5 procedures scheduled including a skin graft to a hand due to delayed wound closure, schwannoma(muscle tumor) removal from an arm and fingers, and an abscess drainage from a young boy’s leg. Without being derogatory or defaming in any particular sense, I was surprised to find the nursing to be insufficient, slow, and without any urgency. This results in the surgeon essentially managing everything, including grabbing instruments, managing anesthesia, drips, and vitals. It was really an excellent example of true surgical mastery. Before the last procedure (a hernia repair), a pregnant patient was wheeled into the opposite theatre. The story was she had failed to progress in labor, stalling at 6cm. They were preparing to do a cesear when I asked how the baby was on CTG (cardiotocography- i.e. Fetal heart rate tracing for my American medical colleagues). “Normal and reassuring,” was the response from the physician. “What is she dilated to?” I asked hesitantly as I was sure this had already been discussed. “She was a 6 about an hour ago,” the midwife said frustratingly. Puzzled, I put a glove on and found the patient to be 10cm, fully effaced, and +1 station! (Non-medical translation- she was ready to have a baby!) I asked for the CTG and was handed a small bluish-green plastic thing. Befuddled and confused, I suddenly realized what this was: a fetoscope! It’s a stethoscope for a fetus’ heartbeat! I’d never used one. I was so excited, and the fellow physician snapped one of my favorite pics to date. The patient was taken back to the ward and delivered without complication.

Using the fetoscope with Dr. Fredlund in the background!
On Friday, I volunteered to present on hypothyroidism and it’s relationship with pregnancy. I will admit that this was an already prepared Neonatal Grand Rounds presentation but I attempted to make this relevant to this community. The decision was made to focus on 3 primary things. 1) HAART medications and safety profiles in pregnancy 2) History of iodide supplementation and it’s effect on decreasing rates of congenital hypothyroidism 3) Including thyroid studies as a part of a recurrent miscarriage workup. Some of you may be aware, but I tend not to read off of my slides; I’m interactive! I’m afraid the medical students who were present were slightly taken aback initially. However, after we settled in, the presentation went smoothly and they even asked for a copy of it afterwards.

Hypothyroidism presentation

Presentation #2
On Saturday evening, a group of 9 arrived for dinner at the Fredlund’s home. To this point, I have tried to stay away from making them the story of this blog. This has become increasingly difficult. They are in a phrase; the definition of giving. Victor Fredlund came to South Africa as a mission doctor straight after internship in London. He came with his wife Rachel who was trained as a social worker. They married in 1977.
The Fredlund’s in 1977

The Fredlunds

The man and his hat
Dr. Fredlund graduated from St. Georges Medical School, part of London University in 1979. His wife Rachel obtained a bachelors in History at Royal Holloway College London University and obtained a Master’s in Social Work at Bedford College London University. After his internship at St. Heliers, Shalton, and The Mother’s Hospital as a General Practioner, they moved to this area in 1981 as missionaries. Along with there new 5 month old (one of three in total), Victor and Rachel realized there were many social challenges and began project after project to deal with each. To date, there are too many to mention throughout the years, however a random example is as follows:
- Christoph Meyer Maths and Science Foundation– offers young people who have performed poorly in maths and sciences to improve and better themselves through dedicated learning, interactive experiments, and specialized/dedicated teachers.
- Vuka Mabasa– started in 1989; instrumental in placing the first reticulated/piped water in the surrounding community, toilets and sanitation, halls for meeting, helps address poor teacher education in maths and sciences.
- Mseleni Care and Compassion Ministries- includes Mseleni Children’s Home, Ebenezer Early Childhood Development Center, and Lulisandla Kumntwana(Reach Out to the Child). A community project working with orphaned and vulnerable children, unemployed youth, and youth in general giving psychosocial support, practical aid, accessing tertiary education, and lifeskills training to equip them for life.
- African Evangelical Church and specifically, Hlulabantu AEC– this was a branch specifically “planted” by the Fredlund’s and now regularly serves anywhere from 50-100 members which come from miles around.

Me hanging a sign for the ECDC for Nelson Mandela Day. On this day, everyone in South Africa donates 67 minutes for volunteerism!
I like how the following was put in a 2016 South African article and will include here:
“His home was never going to be his own: he has probably had 50+ children from the local community live in his house semi-permanently over the 35 years he has been serving the community. Some staying only for months, others for years. Most of these children they nursed through the challenges that kids from broken homes and destitute backgrounds face. Disappointments, suffering, heartaches and tears seem to never be far off from the lives he has chosen to mix his with. Together they have sponsored the school/university fees and living expenses of countless children – a small cost, compared to the huge challenge of keeping the lives of the young people growing up in his house on the path of life. Not only does he have several local children at his table every night but almost always a mix of foreign students or volunteers or anybody else who needs a bed for the night. It’s a conservative estimation to say they probably put up at least one hundred and fifty people per year in their large wooden house –which he built himself!”
Back to the 9 who had come as a part of CoCo’s Foundation(who partners with Mseleni Care and Compassion Ministries). They come to this area to help build homes for orphaned and families in need. After dinner, we gathered in the seating area and began discussing about church the following morning. After 1 cup of coffee and a little nudging, I was asked if I would sing. Dr. Fredlund plays a guitar and regularly sings, and Rachel has a lovely voice and commonly sings as well. I obliged and what occurred was a life-altering experience that I shall remember forever.

Hlulabantu Church prior to service

People starting to arrive from the surrounding villages. The church was quite plain, but lovely nonetheless.

Victor preaching with his guitar
Loading the video of our song here was too large for the blog, so I encourage you to check out the link to it on YouTube. If you get a mere 5% of the joy this gave me, it will be worth a view.

Sorry, comments for this entry are closed at this time.