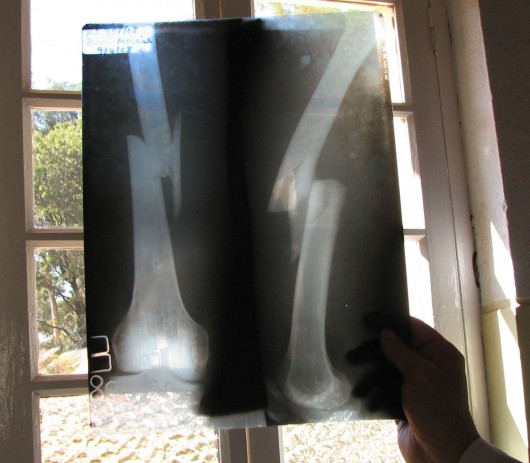
I’m holding up to the window a plain X-ray (remember those?) from a young man in acute pain that fell from a moving bus in Angola, southern Africa. As you can see, the femur fracture is displaced and shortened. As you cannot see, this is also an open fracture. Bony fragments have pierced the skin of his thigh. Beyond pain control and initial debridement, how would you manage this man’s orthopedic injury?
Since the 1970s surgical fixation of such fractures with an intramedullary nail inserted into the femur has the standard of care. Fracture healing from this procedure is rapid and effective, with union rates of between 95% and 99%. However, in the face of an open fracture such procedures in the immediate setting must be delayed until infection risk has suitable declined. And, in this particular African locale no orthopedic or anesthesia specialist is available.

The general approach to such management is monitored traction. A Steinmann pin is inserted just below the tibial tubercle at the time of admission or after initial debridement of the open fracture wounds. Traction beginning with 7 to 8 kg is applied, with the foot of the bed elevated to prevent the patient from sliding forward. Follow up evaluation of the fracture every few days is necessary to assess bony reduction and adequacy of alignment.
Over the ensuing weeks traction should be intermittently lifted to allow the still non-weight bearing patient to mobilize the knee and lessen the risk of joint contracture. After 8-12 weeks of bed rest, and assurance of new bone formation at the fracture site, traction can be suspended and the patient encouraged to begin progressive weight bearing and rehabilitation from the muscle atrophy associated with prolonged immobilization.
Reference: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2266653/